
Not all bad reactions to medicine are the same
You took a pill, and now you feel sick. Maybe your stomach churns, your skin itches, or you can’t breathe. Your first thought? "I’m allergic." But that’s not always true. In fact, most people who think they’re allergic to a medication aren’t. The truth is, there are three very different kinds of bad reactions: side effects, allergic reactions, and intolerance. Mixing them up can cost you time, money, and even your health.
Side effects: the predictable, not-dangerous kind
Side effects are the body’s normal, expected response to how a drug works. They’re not your immune system attacking anything. They’re just the drug doing its job - and a little too well.
Take NSAIDs like ibuprofen. They reduce pain and inflammation by blocking certain enzymes. But those same enzymes also protect your stomach lining. So nausea, upset stomach, or heartburn? That’s a side effect. It’s not dangerous for most people, and it often fades after a few days. Same with drowsiness from antihistamines or nausea from metformin. These aren’t signs your body hates the drug. They’re just side notes in how it works.
Doctors know these reactions because they’re listed in the drug’s official labeling. About 25-30% of people on NSAIDs get stomach issues. 40% of people taking older allergy meds like diphenhydramine feel sleepy. These aren’t rare. They’re common. And they’re not allergies.
Allergic reactions: your immune system sounds the alarm
An allergic reaction is different. It’s your immune system mistaking the drug for a threat - like a virus or pollen - and launching a full attack. This isn’t about how the drug works. It’s about your body’s overreaction to it.
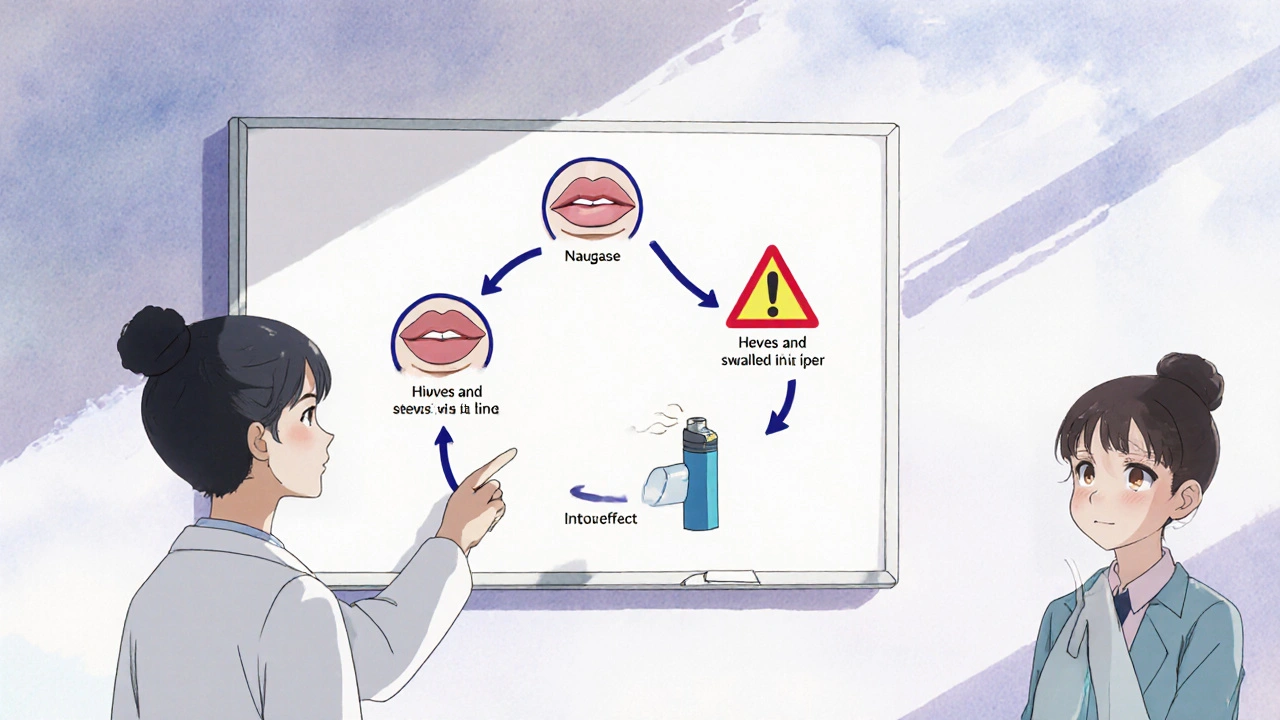
True drug allergies show up fast. Within minutes to an hour after taking the pill, you might break out in hives, your lips or tongue swell, your throat tightens, or your blood pressure drops. These are signs of anaphylaxis - a medical emergency. You might need epinephrine. You might need an ambulance.
Only 5-10% of all bad drug reactions are true allergies. Yet, 10% of Americans say they’re allergic to penicillin. Only 1% actually are. That’s a 90% error rate. People say they’re allergic because they got a rash or threw up after taking amoxicillin. But rashes from viruses? Vomiting from stomach upset? Those aren’t allergies. They’re side effects.
Real allergies usually get worse with each exposure. If you had a mild rash after penicillin once, and then got a full-blown anaphylactic reaction the second time? That’s your immune system remembering. That’s not a side effect. That’s an allergy.
Intolerance: your body just can’t handle it
Intolerance is the middle ground. It’s not an immune response. But it’s not just a common side effect either. It’s your body being unusually sensitive to a drug’s effects - even at normal doses.
Take aspirin or ibuprofen. Most people take them without issue. But about 7% of adults with asthma develop breathing problems, nasal polyps, or wheezing after taking them. That’s not an allergy. It’s intolerance. Their bodies react badly to the way these drugs block certain enzymes. They can’t tolerate it, even though the drug is working exactly as designed.
Another example: codeine. Most people take it for pain and feel fine. But 7% of Caucasians have a gene variation that turns codeine into morphine too fast. They get extreme nausea, dizziness, or even trouble breathing - not because they’re allergic, but because their body makes too much of the active drug. That’s intolerance.
Unlike allergies, intolerance doesn’t mean you’re at risk for anaphylaxis. But it does mean you need to avoid that drug - or switch to a different one. Celecoxib, for example, doesn’t trigger the same reaction in people with aspirin intolerance because it works differently.
Why it matters: mislabeling can kill
Calling a side effect an allergy sounds harmless. But it has real consequences.
If you’re labeled "allergic to penicillin," doctors avoid it. They give you stronger, more expensive antibiotics instead. Those drugs are less effective against common infections. They’re more likely to cause C. diff - a dangerous gut infection. They increase your risk of MRSA. Studies show people with mislabeled penicillin allergies have 30% higher rates of C. diff and 50% higher rates of MRSA.
And it’s not just antibiotics. A 2021 study found mislabeling adds $2,500 per patient per year in extra costs. Hospitals spend more. Patients stay longer. Surgeries get delayed. One patient avoided all antibiotics for 15 years because she thought she was allergic after getting nauseous once. She later got tested - and found out she wasn’t allergic at all. Since then, she’s taken amoxicillin eight times without issue.
Every year, over 1,200 medication errors in the U.S. happen because someone was wrongly labeled allergic. That’s not just a mistake. It’s a public health problem.
How to tell them apart: a simple guide
Here’s how to spot the difference:
- Side effect: Nausea, dizziness, headache, dry mouth, drowsiness. Starts within hours. Gets better with time or lower dose. Happens to many people. Doesn’t get worse with repeat use.
- Allergic reaction: Hives, swelling of face/lips/tongue, wheezing, trouble breathing, rapid heartbeat, passing out. Starts within minutes to an hour. Gets worse with each exposure. May need epinephrine. Involves immune system.
- Intolerance: Severe reaction at normal dose - like asthma flare-up from NSAIDs, extreme vomiting from codeine. Not immune-related. Doesn’t happen to most people. Avoidance is needed, but not because of anaphylaxis risk.
What to do if you think you’re allergic
If you’ve ever had a reaction, don’t assume it’s an allergy. Write down what happened:
- What drug? When did you take it?
- What symptoms? How long after?
- Did you need emergency care? Epinephrine? Hospitalization?
Then, talk to your doctor. Ask: "Could this have been a side effect or intolerance?" If your reaction involved breathing trouble, swelling, or required epinephrine, ask for a referral to an allergist. They can do skin tests or a controlled challenge to confirm.
Penicillin allergy testing is now routine in many hospitals. The CDC recommends it for anyone with a label. The test takes about 3 hours. Results are over 95% accurate. And if you’re cleared? You can safely use penicillin again - and avoid unnecessary, riskier antibiotics.

What to tell your doctor
Don’t say, "I’m allergic to penicillin." Say:
- "I got diarrhea after taking amoxicillin." → That’s a side effect.
- "I broke out in hives 20 minutes after taking penicillin and my throat closed." → That’s a true allergy.
- "I get asthma attacks when I take ibuprofen." → That’s intolerance.
Be specific. Use exact words. Document it right. Your doctor needs to know the difference to keep you safe.
What’s changing in medicine
Hospitals are catching on. The CDC’s "Get Smart" campaign has helped cut penicillin allergy labels by 30% in clinics that test patients. Electronic health records now flag when a patient says "allergy" but describes a side effect - and prompt doctors to double-check.
In 2023, the FDA launched a program using AI to scan millions of medical records for mislabeled allergies. Researchers are testing a 15-minute penicillin test that could replace the 3-hour version. And in 2025, a simple clinical tool called PEN-FAST may let doctors safely skip testing for low-risk patients.
Long-term? If we fix this problem, the U.S. could save $18.4 billion a year by 2030. Fewer infections. Shorter hospital stays. Better antibiotics. Better care.
Bottom line
Feeling sick after a pill doesn’t mean you’re allergic. Most of the time, you’re not. Side effects are common. Intolerance is real but rare. True allergies? Very rare. But they’re life-threatening.
Don’t assume. Don’t self-diagnose. Don’t let a 10-year-old stomach ache keep you from the right medicine. If you’re unsure, get tested. Your next prescription - and maybe your life - depends on it.



Comments
Erika Hunt
Okay, so I’ve been taking ibuprofen for years, and yeah, I get the stomach thing - but I just chalked it up to ‘oh, I ate too fast’ or ‘coffee on an empty stomach.’ Now I’m realizing it’s not just me being a mess; it’s literally the drug blocking protective enzymes. I mean, I didn’t know that was normal for 25-30% of people? That’s like… one in four. Why isn’t this on the bottle? Why isn’t it in the ads? Why do we just assume nausea = ‘you’re weak’? I feel like pharmaceutical companies don’t want us to know the difference between side effect and allergy because then we’d stop self-diagnosing and start asking for tests. And honestly? I’m kind of mad I didn’t get tested after my rash in college. Could’ve saved me a decade of avoiding penicillin for nothing.
Sharley Agarwal
Allergy? No. Just weak body.
prasad gaude
You know, in India, we have this phrase - ‘dawa ka asar’ - the effect of the medicine. We don’t always separate side effect from allergy. We just say, ‘this pill made me feel bad.’ But this article? It’s like a quiet revolution. We’ve been blaming our bodies for decades. But the body isn’t broken - the labeling is. I’ve seen a cousin take codeine and collapse from nausea - family said ‘allergy.’ But it was her genes. Fast metabolizer. Now she takes tramadol. No drama. No panic. Just science. Maybe we need to stop treating medicine like a curse and start treating it like a conversation. Your body talks. You just have to learn the language.
Jennifer Griffith
so like... i took amoxicillin once and got a rash. now i'm allergic. right? lol no but like... i think i am?? idk i'm just scared now.
Patricia McElhinney
It is both scientifically and ethically indefensible that 90% of penicillin allergy labels are inaccurate. The persistence of this misinformation is a direct result of systemic negligence in medical education and patient counseling. The CDC’s data is unequivocal: misclassification leads to increased morbidity, mortality, and healthcare expenditure. To continue allowing patients to self-diagnose drug reactions without objective testing is not merely negligent - it is criminal. Hospitals must implement mandatory allergy re-evaluation protocols. Every patient labeled ‘penicillin allergic’ must be referred to an allergist within 30 days of documentation. This is not a suggestion. It is a public health imperative.
Rachel Villegas
I used to think my hives after penicillin meant I was allergic. Turned out it was a virus I had at the same time. Got tested last year - negative. Now I take amoxicillin like it’s candy. My doctor was like, ‘We see this all the time.’ Honestly? I’m embarrassed. But also… relieved. I wish I’d known this 15 years ago. If you think you’re allergic, get tested. It’s not a big deal. Three hours. Maybe a little pinch. Worth it.
Aki Jones
Let’s be real - this isn’t about medical accuracy. It’s about control. Who benefits from keeping people afraid of penicillin? Pharma. Big Pharma. Why? Because the alternatives - vancomycin, clindamycin, azithromycin - are 10x more expensive. And guess what? They’re all linked to C. diff. And MRSA. And antibiotic resistance. The FDA’s ‘AI scanning’ program? That’s PR. They’re not fixing the system. They’re just making it look like they care. Meanwhile, hospitals still let nurses write ‘allergy’ in charts based on a patient saying ‘I threw up once.’ That’s not medicine. That’s laziness dressed up as protocol. And the real tragedy? People are dying because someone didn’t bother to ask, ‘When exactly did the rash appear?’
Jefriady Dahri
Bro, I had this friend in college - took ibuprofen, got asthma attack. Thought he was allergic. Never took it again. Five years later, he goes to a clinic, gets tested - turns out he had exercise-induced asthma and the ibuprofen just made it worse. He’s been taking it since. No problems. I mean… imagine if he’d just asked? 😅 So yeah - don’t assume. Talk to a doc. Get tested. Your future self will high-five you. 🙌
Timothy Sadleir
There’s a deeper truth here: we’ve outsourced our bodily intuition to labels. We don’t listen to our bodies anymore - we Google symptoms and then we slap on a diagnosis like a sticker. ‘I’m allergic.’ ‘I’m intolerant.’ ‘I’m sensitive.’ But we never ask: why? What changed? When did this start? Who told me this was real? The truth is, most of us don’t know what our bodies are telling us. We just want a quick answer. And medicine, in its infinite wisdom, gives us one - even if it’s wrong. Maybe the real epidemic isn’t mislabeled allergies… it’s the loss of curiosity about our own physiology.
Dolapo Eniola
USA think they know everything about medicine. In Nigeria, we know: if medicine make you sick, you don’t take again. No test. No doctor. Just wisdom. You think your penicillin test is advanced? We have grandma’s tea and prayer. And guess what? We don’t have 1,200 medication errors a year. We have respect. You over-medicalize everything. We just survive. 😎
Agastya Shukla
Interesting how intolerance is often genetic - like the codeine CYP2D6 polymorphism. That’s pharmacogenomics 101. But we don’t screen for it. Why? Cost. Accessibility. Bias. If you’re white and from the West, you might get tested. If you’re from a low-income background? You get labeled ‘allergic’ and switched to a broader-spectrum antibiotic. This isn’t just about terminology - it’s about equity in precision medicine. We need population-specific pharmacogenomic databases. And we need to stop assuming that ‘common side effects’ are universal. They’re not. Biology is regional. Culture is not a substitute for genetics.
Josh Zubkoff
Okay, so let me get this straight - the entire U.S. healthcare system is built on a 90% error rate? People are being denied penicillin because they threw up once? And we’re okay with that? And now we’re spending billions on AI to scan records that were filled out by nurses who didn’t even read the patient’s notes? This isn’t a medical issue. This is a systemic collapse. And the worst part? The people who suffer the most? They’re the ones who can’t afford to get tested. The ones who can’t take time off work. The ones who don’t have insurance that covers allergists. So we just keep giving them vancomycin and calling it ‘care.’ And we pat ourselves on the back for being ‘evidence-based.’ Meanwhile, someone’s kid is in the ICU because they got C. diff from a drug they didn’t even need. This isn’t just negligence. It’s a moral failure.
Leisha Haynes
so you're telling me i didn't need to avoid all NSAIDs because i got a headache once? wow. my life is a lie.
Shivam Goel
Let’s not forget: the term ‘intolerance’ is often misused to downplay real reactions. In clinical practice, we’ve seen patients with NSAID-induced asthma mislabeled as ‘just sensitive’ - then they end up in the ER with status asthmaticus. The distinction between side effect and intolerance matters - but the distinction between ‘mild’ and ‘life-threatening’ matters more. Intolerance isn’t ‘minor.’ It’s a clinical red flag. And if your doctor dismisses it because ‘it’s not an allergy’ - find a new doctor. This isn’t semantics. It’s survival.
Erika Hunt
Wait - I just read the part about PEN-FAST. That’s actually kind of genius. A clinical tool that lets doctors skip testing for low-risk patients? That’s not just efficient - it’s equitable. It means someone in rural Alabama won’t have to drive three hours to an allergist just to get cleared for amoxicillin. And if it reduces unnecessary antibiotic use by even 10%? That’s a win. I used to think testing was only for ‘serious’ cases. But now I see it’s for everyone. Even me. Even the person who just got a little tummy ache. Because if we don’t fix the labeling, we’re just passing down fear like a family heirloom.